Donald P. Becker, M.D.
Indications
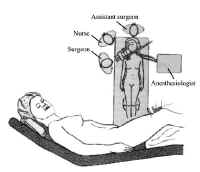 Figure 1: Patient position for transsphenoidal approach.
Figure 1: Patient position for transsphenoidal approach.
The transsphenoidal approach is the procedure of choice for the removal of tumors of the sella that are still largely confined to this space. It is also indicated for removal of some tumors of the parasellar area. Pituitary tumors with substantial intracranial extension can engulf important structures and should be treated using a transcranial approach.
For transsphenoidal surgery, there are several alternative approaches to the sphenoid sinus. These include the transnasal paraseptal, sublabial-transseptal, and paranasal transethmoidal approaches. For processes that are largely located in the sella, the sublabial or trananasal approach is used. With extreme involvement of the paranasal sinuses, the paranasal transethmoidal exposure is of benefit.
Position
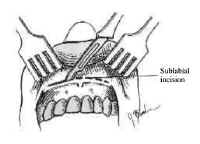 Figure 2: Sublabial incision.Proper positioning is essential in transphenoidal surgery to ensure adequate expsure of the sphenoid sinus structures, to minimize bleeding, and to maximize the surgeons comfort It is also crucial in helping to ensure that the operative dissection remains midline.
Figure 2: Sublabial incision.Proper positioning is essential in transphenoidal surgery to ensure adequate expsure of the sphenoid sinus structures, to minimize bleeding, and to maximize the surgeons comfort It is also crucial in helping to ensure that the operative dissection remains midline.
The patient is positioned supine with the head elevated to 30 degrees, turned 20 degrees toward the surgeon, and flexed toward the opposite shoulder (Figure 1).
The head is placed in a head immobilizer or, alternatively, supported with a padded ring. We prefer the latter because this allows subtle movement of the operative field intraoperatively without the need for microscope repositioning. The nurse stands next to the surgeon, and the patient is positioned at the head of the table (see Figure 1).
Operative Procedure
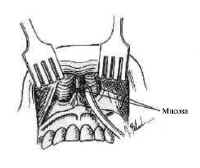 Figure 3: Elevation of the inferior mucosa within each aperture.We describe in this chapter the sublabial approach for transsphenoidal surgery.
Figure 3: Elevation of the inferior mucosa within each aperture.We describe in this chapter the sublabial approach for transsphenoidal surgery.
A sublabial incision positioned on the gingival mucosa well above the teeth is made extending between the canine teeth (Figure 2).
Periosteal elevators are used to elevate the mucosa off the maxilla. After the pyriform apertures are identified and defined, the inferior mucosa within each aperture is elevated along the premaxilla, forming inferior tunnels (Figure 3).
The cartilaginous septum is exposed using sharp dissection, and a submucosal tunnel is -elevated along its left side. Fibrous adhesions at the base of the cartilage must be divided sharply, allowing the septum to be disarticulated from the nasal spine and maxilhry ridge. The cartilage can then be hinged to the patients right side. Increased exposure may require enlargement of the pyrlibrm apertures with rongeurs or removal of the nasal spine (Figure 4).
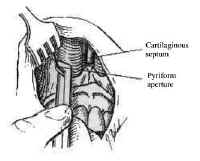 Figure 4: Enlargement of the pyriform apertures.Posteriorly, the mucosa is elevated from both sides of the bony septum, which subse quendy is fractured, removed, and saved. Under microscopic magnification, the characteristic keel appearance of the vomer is seen during this phase (Figure 5).
Figure 4: Enlargement of the pyriform apertures.Posteriorly, the mucosa is elevated from both sides of the bony septum, which subse quendy is fractured, removed, and saved. Under microscopic magnification, the characteristic keel appearance of the vomer is seen during this phase (Figure 5).
The anterior wall of the sphenoid sinus is confirmed by identifying the ostea, located superolaterally, or with a lateral radiograph. The sinus is opened widely, and all mucosa is removed from within it to prevent trouble some bleeding. Placement of the speculum within the sphenoid sinus should be avoided because fracture of the sphenoid bone can result in injury to the optic nerve, cranial nerves, and carotid artery. After the mucosa is removed, the bulge of the sella is readily apparent and, typically, is thinned by the tumor. If necessary, the- bone of the sella can be fractured with a small osteotome or removed wid1 a diamond drill, exposing the medial extent of each cavernous sinus (Figure 6). In rare cases, the sphenoid sinus is incompletely pneumatized, requiring removal of bone with a high speed drill to expose the sella.
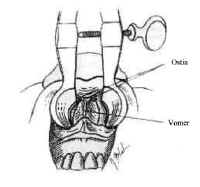 Figure 5: Visualization of the characteristic keel of the sphenoid sinus.The dura is incised in a cruciate manner after coagulating it with the bipolar electrocautery. Intercavernous venous channels that extend across the sella frequently result in brisk bleeding when the dura is incised The bleeding can be controlled by grasping both, leaves of the dura with the bipolar forceps and coagulating.
Figure 5: Visualization of the characteristic keel of the sphenoid sinus.The dura is incised in a cruciate manner after coagulating it with the bipolar electrocautery. Intercavernous venous channels that extend across the sella frequently result in brisk bleeding when the dura is incised The bleeding can be controlled by grasping both, leaves of the dura with the bipolar forceps and coagulating.
Pituitary adenomas usually are soft and can be readily removed with bayonetted ring curettes. Intermittent. Valsalva maneuvers by the anesthesiologist expedite tumor removal by elevating the subarachnoid fluid pressure, which is transmitted to the tumor capsule, displacing tumor tissue downward.
After the bulk of the tumor is removed, the sella is inspected systematically and the pituitary gland itself is examined. If the tumor capsule prolapses into the sphenoid sinus or cerebrospinal fluid leakage occurs, fascia lata or adipose tissue and fibrin glue may be used to occlude the communication to the subarachnoid space and support the diaphragma sellae. The floor of the sella can be reconstructed vvith the bony septum previously removed. After complete hemostasis is achieved, the speculum is removed and the sublabial mucosa is closed with interrupted absorbable structures.
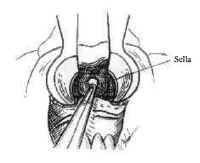 Figure 6: Removal of the floor of the sphenoid sinus.Petroleum jelly-covered gauze is packed into each nasal passage and left in place for 48 to 72 hours.
Figure 6: Removal of the floor of the sphenoid sinus.Petroleum jelly-covered gauze is packed into each nasal passage and left in place for 48 to 72 hours.
In the case of extensive dural defect, lumbar cerebrospinal fluid drainage for 2 to 3 days is advisable.
Cavernous Sinus Extension of Tumors
Some tumors extend in the lateral direction, requiring surgicalentry into the medial cavernous sinus. In these cases, the surgeonmust be familiar with the important anatomical structures adjacentto the sella before proceeding with surgery. The structures mostat risk include the internal carotid artery and its intracavernousbranches as well as cranial nerves to extraocular muscles.
Sometimes better exposure of the medial wall of the sphenoidsinus and cavernous sinus is necessary in these situations Thiscan be gained by enlarging the pyriform aperture or by removingthe medial maxillary sinus wall contralateral to the involvedcavernous sinus and directing the speculum laterally.
Tumors that involve the medial cavernous sinus typicallyobliterate the venous channels and can be removed piecemeal usingmicrodissectors. These instruments can be gently used to removethe tumor around the carotid artery with special care to avoidinjury to the ocular muscle nerves, particularly the abducensnerve.
Significant venous bleeding is not a problem until the finalstages of tumor removal as the patent part of the sinus isexposed. As with other approaches to the cavernous sinus, thetumor should be removed in an organized manner and bleedingcontrolled with carefully placed oxidized cellulose and pressure.
Recommended Reading
Balagura, S., Tindall, G.: Technique of transsphenoidalMicrosurgery. Contemp. Neurosurg. 3(24): 1982.
Eisele, D., Flint, P., Janas, J., et al.: The sublabialtransseptal transsphenoidal approach to sellar and parasellarlesions. Laryngoscope 98:1301-1308,1988.
Tindall, G., Herring, C., Clark, R., et al.: Cushingsdisease: Results of transsphenoidal microsurgery with emphasis onsurgical failures. J. Neurosurgery. 72:363-369, 1990.
Tucker, H., Hahn, J.: Transnasal, transseptal sephenoidalapproach to hypophysectomy. Laryngoscope 92:55-57, 1982
Welbourn, R.: The evolution of transsphenoidal pituitarymicrosurgery. Surgery 100(6):1185-7789, 1986