Highlights Newsletter
PNA Highlights July 2026
“Wellness is the complete integration of body, mind, and spirit – the realization that everything we do, think, feel, and believe has an effect on our state of well-being.” – Greg Anderson
PNA Spotlight: Dr. Pouneh Fazeli
Endocrinologist Dr. Pouneh Fazeli is Chief of the Division of Endocrinology and Metabolism at the University of Pittsburgh School of Medicine. She did her undergraduate work at Harvard University and earned her medical degree from the University of Pennsylvania. She did a residency and then a chief residency at Columbia University Medical Center, as well as a fellowship in Endocrinology at Massachusetts General Hospital. Dr. Fazeli was kind enough to answer a series of questions from the PNA; her answers follow.
What is your current position?
I am Chief of the Division of Endocrinology and Metabolism at the University of Pittsburgh School of Medicine. I moved to UPMC in 2019 to start the Neuroendocrinology Unit. Together with our outstanding neurosurgical and multidisciplinary teams, we started a Pituitary Center of Excellence.
Please describe your educational journey and mentors
I really fell in love with pituitary physiology and pathophysiology as a medical student at the University of Pennsylvania. I rotated in Dr. Peter Snyder’s clinic, and he is a renowned neuroendocrine pituitary specialist. After seeing patients with him as a third-year medical student, I decided I wanted to become a pituitary endocrinologist. I was a resident in internal medicine and a chief resident at Columbia University Medical Center, where I worked with wonderful endocrinologists, including Drs. Sharon Wardlaw and Pamela Freda. When I did my fellowship at Mass General Hospital, my primary mentor was Dr. Anne Klibanski. I also worked with outstanding clinical mentors including Drs. Lisa Nachtigall and Beverly Biller.
Read More Here
How Precision Tools Are Improving Pituitary Surgery
Pituitary surgery requires a careful balance: removing the tumor while protecting the normal pituitary gland, optic nerves, carotid arteries and nearby brain structures. Today, Mayo Clinic researchers are helping move the field toward more precise care—guided by better imaging, improved diagnostic tools and real-time support in the operating room.
The goal is straightforward but difficult to achieve: find the tumor more accurately, plan surgery more safely, and personalize care before, during and after treatment.
A clearer map for hard-to-see Cushing tumors
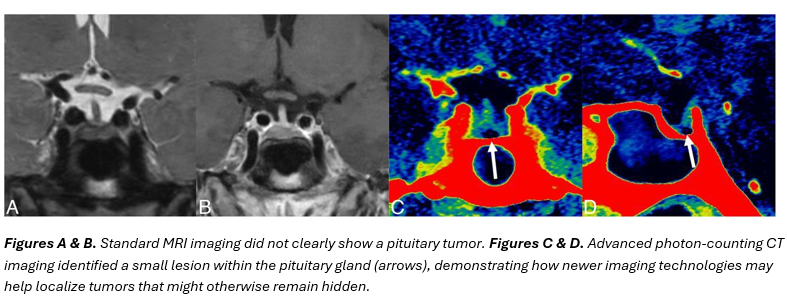
For patients with Cushing disease, precise tumor localization remains one of the greatest challenges. Tumors that produce excess adrenocorticotropic hormone (ACTH) are often extremely small and can be difficult to visualize on standard MRI.
In this recent study, Mayo Clinic radiologist Dr. Ian Mark, neurosurgeon Dr. Jamie Van Gompel and collaborators evaluated an advanced imaging technology called photon-counting detector CT (PCD-CT). Unlike standard MRI, PCD-CT can capture much finer anatomical detail, allowing clinicians to see tiny structures within the pituitary gland more clearly.
In 25 patients with Cushing disease, PCD-CT localized tumors in 92% of cases, compared with 56% using standard MRI.
For patients, this matters because greater localization may allow surgeons to perform a more targeted operation, rather than having to explore more of the gland. The study does not mean PCD-CT should replace MRI, but rather, it points to an important future role for advanced imaging, especially when MRI can leave uncertainty.
A new perspective on calcified masses
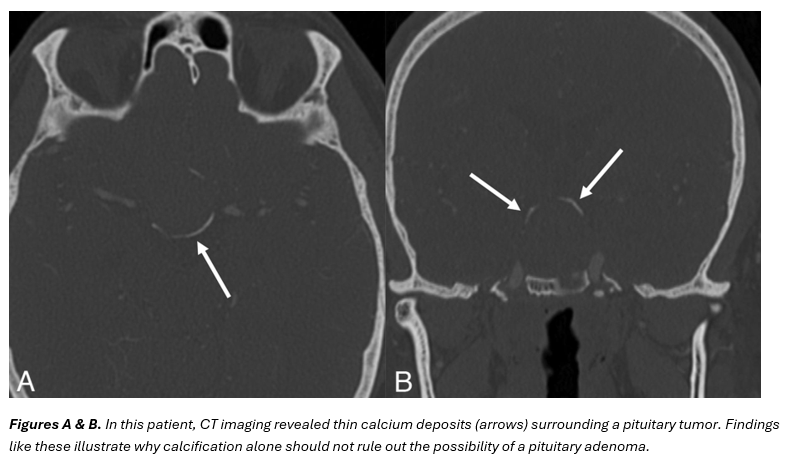
Another facet of precision care involves making the correct diagnosis before surgery. Large sellar or suprasellar masses with calcification—small deposits of calcium that appear as hardened areas on imaging scans—have traditionally raised concern for craniopharyngioma, a rare tumor that develops near the pituitary gland and often requires a different surgical strategy than a pituitary adenoma.
Because calcification is commonly seen in craniopharyngiomas, its presence on imaging has traditionally been considered a hallmark of that diagnosis. However, a recent Mayo Clinic study found that calcification is not exclusive to craniopharyngiomas.
After reviewing 45 pathology-confirmed giant pituitary adenomas, researchers found that 22% contained calcifications. These findings challenge a longstanding assumption and further suggest that calcification alone should not rule out a pituitary adenoma or automatically determine a diagnosis.
For patients, this is another example of precision medicine in action. A more accurate diagnosis helps surgical teams better understand what type of tumor they are treating, consider all appropriate treatment options and develop a care plan tailored to the individual patient.
Using prolactin as a clue before surgery
When considered alongside imaging and other clinical information, blood test results can also help guide a more precise treatment plan.
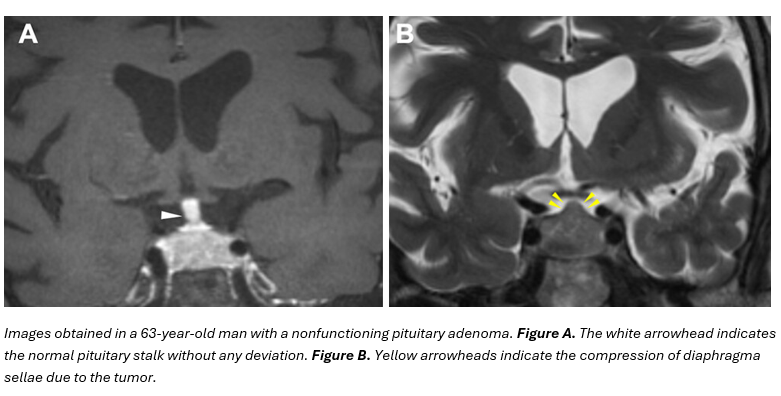
In a study involving Mayo Clinic researchers, patients with nonfunctioning pituitary adenomas—tumors that do not produce excess hormones—provided a preoperative blood sample.
Among 244 patients, 54% had elevated prolactin levels before surgery. This is often called the “stalk effect.” As a tumor grows, it can put pressure on the pituitary stalk—the connection between the brain and the pituitary gland—disrupting normal hormone signals and causing prolactin levels to rise.
The study suggests that elevated prolactin may serve as an early warning sign that the pituitary gland is already under stress. Patients with higher prolactin levels were also more likely to experience certain hormone deficiencies after surgery, including issues involving thyroid hormone production and the body’s ability to make cortisol, a hormone that helps regulate stress, blood pressure and energy levels.
While elevated prolactin does not guarantee that hormone dysregulation will occur, it may help doctors identify patients who could benefit from closer hormone monitoring and tailored follow-up care after surgery.
Real-time guidance in the operating room
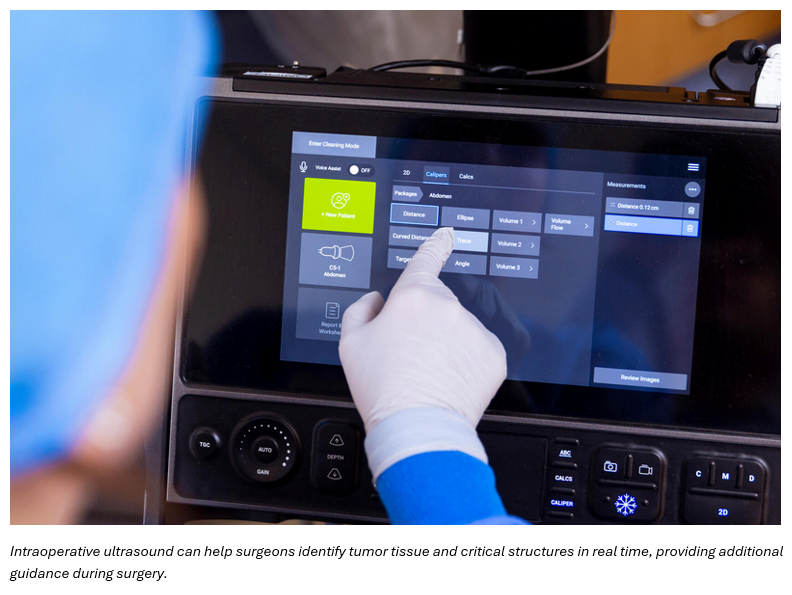
Finally, precision surgery also depends on what happens during the operation itself. In this editorial on intraoperative ultrasound, Drs. Jamie Van Gompel and Hamid Borghei-Razavi discuss renewed interest in using ultrasound during pituitary surgery.
One of the biggest challenges surgeons face is distinguishing tumor tissue from the normal pituitary gland while operating. Although preoperative imaging is essential for planning surgery, anatomy can shift as tumor removal progresses, making those images less reliable in real time.
Intraoperative ultrasound may help bridge that gap by providing surgeons with live imaging during the procedure.
This technology can help identify tumor tissue, look for any remaining tumor and avoid critical brain structures. It may be especially valuable when tumors are difficult to visualize on MRI. Because ultrasound is portable, does not use radiation and can be incorporated directly into the surgical workflow, researchers believe it has the potential to become an important tool for improving surgical precision and safety.
A clearer path forward
Together, these studies show that precision pituitary surgery is not one single technology. It is a broader movement toward improved imaging before surgery, stronger indications from lab tests, and greater guidance in the operating room.
For patients, the message is hopeful but practical: not every tool is right for every case, and several of these approaches still need further validation. But if imaging is unclear, surgery feels complex or follow-up planning is uncertain, it may be worth asking your care team whether advanced imaging, specialized pituitary review or additional endocrine monitoring could be appropriate.
Learn more about pituitary tumor care at Mayo Clinic and explore available diagnostic and treatment options.
PNA Medical Corner: Infection-related Hospitalization and Cushing’s Syndrome
This month the PNA Medical Corner showcases a study coauthored by PNA member Dr. Maria Fleseriu, an
 endocrinologist at Oregon Science and Health University. They conclude that patients they studied with Cushing’s Syndrome ended up in the hospital due to infection more than twice as often as people in the control group.
endocrinologist at Oregon Science and Health University. They conclude that patients they studied with Cushing’s Syndrome ended up in the hospital due to infection more than twice as often as people in the control group.
Am J Med 2026 Jun 24:S0002-9343(26)00495-X.
doi: 10.1016/j.amjmed.2026.06.017. Online ahead of print.
Risk of Infection-Related Hospitalization Is More Than Doubled in Cushing’s Syndrome vs Matched Controls
Amit Akirov 1, Alaa Atamna 2, Yaron Rudman 3, Shiri Kushnir 4, Tzippy Shochat 5, Maria Fleseriu 6
Affiliations Expand
PMID: 42342186 DOI: 10.1016/j.amjmed.2026.06.017
Abstract
Background: Cushing’s syndrome is associated with immune dysfunction and increased susceptibility to infection, yet risk of infection-related hospitalization remains unclear. We evaluated infection-related hospitalization in Cushing’s syndrome versus controls.
Methods: Using the Clalit Health Services database, 609 patients with Cushing’s syndrome were identified and matched to 3,018 controls by age, sex, socioeconomic status, and body mass index. The primary outcome was infection-related hospitalization. Competing-risk models were used with death as a competing event. Analyses were performed according to etiology, remission, and infection subtype.
Results: During mean follow-up of 13.4 years in patients with Cushing’s syndrome and 13.9 years in controls, infection-related hospitalization occurred in 14.1% vs 5.9% (86/609 vs 178/3,018), with incidence rates of 10.5 vs 4.2 per 1,000 person-years. Patients with Cushing’s syndrome had a higher risk of infection-related hospitalization (HR 2.5, 95% CI 1.9-3.2), observed in both Cushing’s disease (HR 3.8, 95% CI 2.5-5.7) and adrenal disease (HR 2.3, 95% CI 1.5-3.6). Respiratory and genitourinary infections were the most common causes, and opportunistic infections were more frequent in Cushing’s syndrome (12.5% vs 5.6%, p=0.04). Patients in remission remained at increased risk (HR 2.5, 95% CI 1.6-3.8), while older age and higher body mass index independently predicted hospitalization, with most infections occurring in patients aged ≥55 years and body mass index ≥25 kg/m².
Conclusion: Patients with Cushing’s syndrome have an excess risk of infection-related hospitalization affecting both common and opportunistic infections and risk persists after remission. These findings support ongoing infection surveillance and preventive measures.
Keywords: Cushing’s Syndrome; Hospitalization; Infection; Pituitary.
Count on your Xeris CareConnection™ Team for unparalleled Cushing’s Support
Cushing’s can be challenging, but there is support so patients can feel like themselves again. The main goal of treating Cushing’s is to get cortisol levels back to normal. This Pituitary Awareness Month, Xeris Pharmaceuticals® is highlighting the importance of one-on-one support for patients living with Cushing’s Syndrome and support for HCPs treating Cushing’s Syndrome.
Sign up to get dedicated support:
Patients: Sign up for support | Recorlev® (levoketoconazole)
HCP’s: Connect with Xeris support | RECORLEV® (levoketoconazole)
Have more questions? Call for more support at 1-844-444-RCLV (7258)
Copyright © 2024 Pituitary Network Association All rights reserved.
Disclaimer: PNA does not engage in the practice of medicine. It is not a medical authority, nor does it claim to have medical expertise. In all cases, PNA recommends that you consult your own physician regarding any course of treatment or medication.
Our mailing address is:
Pituitary Network Association
P.O. Box 1958
Thousand Oaks, CA 91358
(805) 499-9973 Phone - (805) 480-0633 Fax
Email [email protected]
You are receiving this Newsletter because you have shown interest in receiving information about our activities.
If you do not want to receive any more emails from PNA, Unsubscribe.
